

Metastatic Prostate Cancer in Israel: A Brief Case History (Mine)
")
This is a story that is still ongoing, yet is perhaps worth sharing as elements of it may apply to others, directly or indirectly, at points in the future and the experience might be of some value to them.
My family doctor became suspicious of possible prostate cancer following a routine blood test earlier this year, in February, 2019 when a, cancer-indicating, blood marker specific to prostate cancer suggested there could be a significant problem. It is called PSA (Prostate Specific Antigen) and anyone worried about their prostate will hear a lot about it.
A confirming, and frankly quite intrusive, ultrasound guided biopsy in March, organized by a hastily recruited Urologist, indeed showed the presence of aggressive cancer of the prostate, rated 10 on the so-called “Gleason” scale – which is as high as it goes. Then a PET/CT (Positron Emission Tomography/Computed Tomography) scan in April indicated metastasis had begun to spread the cancer elsewhere, though fortunately not yet very far. Therefore, in May I entered the out-patient cancer programme at the Rambam Hospital in Haifa – a teaching hospital which sits right next door to, and is affiliated with, the Technion Medical School.
The treatment plan designed for me by the medical team at the Rambam’s Oncology Centre is intended to lead, if successful, to a complete cure by way of what is called “combination therapy”. This comprises, first, a pharmacological component employing medications over a substantial period of months that suppress the production of testosterone in the body. Testosterone is a necessary presence for the growth of malignant tumours it would seem. In this case the current medication of choice is Zytiga (generic: Abiraterone), with two other similarly acting compounds having played a supporting role as well.
The second component of the combination therapy entails intense irradiation of all the now-known, and some hypothesized by extension, malignant cancerous areas of the body using state of the art radiation equipment, over a period of many weeks.
The testosterone reducing medications began in May, and will continue likely into next summer, and the radiation treatments began in mid-August and were completed recently at the end of October.
The radiation programme began with a number of, essentially intelligence-gathering, preparatory “simulation” scans on CT (defined above) and MRI (Magnetic Resonance Imaging) machines, designed to map out in detail, and then help define with precision the prospective scope, and intensity of subsequent planned intensive radiation treatments. These, combined with the pharmacological solution above, are supposed to kill malignant cancer cells wherever known to have been found up until then, and in certain surrounding areas as well with a decent probability of finding more.
Both the PET/CT and the recent MRI scan also showed the physical outline of the malignant tumour within the prostate itself, something having a total volume of about 20 cubic centimetres. These imaging tools allowed me to, if you like, visualize the face of the enemy – something very personal to me. And when you go to war this helps.
Prostate cancer that has remained confined within the prostate gland can sometimes be relatively (!) benign, and even if more advanced can often be treated by surgical removal. Once it has metastasized beyond the prostate gland itself, however, it becomes much more dangerous if not caught early in that process, and statistics show it can then be seriously lethal.
The radiation treatments, now completed over a two-and-a-half-month period, were as follows:
- First, three SBRT (Stereotactic Body Radiation Therapy) ultra-high intensity radiation sessions targeted at known malignant cancer cells which had attached to the dorsal vertebra D5 (thoracic T5).
- Then, twenty-eight high intensity radiation sessions targeted at known aggressive malignant cancer cells within the prostate itself; at the whole general pelvic area and, as well, at known aggressive malignant cancer cells clustered amongst affected lymph glands in the right Iliac. The Iliac region lies at the junction of the thigh and the lower abdomen, aka the groin.
The machine they used to irradiate the prostate gland, the pelvic area and the affected lymph nodes is a microwave-based Linear Accelerator (Linac) machine – in this case a brand-new Elekta Versa HD unit, one that cost the hospital a number of millions of dollars.
The Rambam has just installed two of these latest-tech machines, one of which I believe can also perform some CT functions. Both are spanking-brand-new, and are located in the hospital’s new Radiation Centre. This is part of a major investment in their new Oncology Centre which was funded substantially by the family of the late Joseph Fishman. They are also installing two more Linac machines there next year as well, for which altogether four, separate, radiation hard-shielded rooms have been prepared. Other existing machines are located in the older parts of the hospital as well, providing overall a well-provisioned resource. The new Radiation Centre is actually placed three floors below ground level to protect from bombing in the event of war. In fact, I believe the whole underground parking lot morphs into an underground hospital itself at such a time, when all patients would be moved down into it – with all the cars removed.
From the internet Elekta appears to be a Swedish company, though one doctor told me it was American and another doctor told me it was English. To irradiate the spine a somewhat smaller existing Elekta Linac machine was utilized.
To assist in synchronizing, precision focused, prostate targeting by the new Linac machine, they first inserted 3 near pure-gold, “Fiducials”, or reference marker “seeds” into my prostate gland, using ultrasound guidance, which I’m told will now stay there for life. To protect surrounding organs from being damaged by the intense radiation they then also inserted a radiation-opaque “spacer” hydrogel, called by the somewhat awkward marketing name “Space OAR”. This was quite expensive, as it is not yet covered by the government health basket (but certainly should be at this point as it clearly did its job). Both procedures were performed under general anaesthesia too (thank goodness).
The technology deployed above is all very much up to date and seems completely state of the art. I know a friend of mine just told me her French father-in-law had to go to Monaco to get exactly the same treatment arrangements some time back – which were successful. The health care system here in Israel is quite progressive, as is Maccabi my local HMO (Health Management Organization), and so-far the standard of the medical care I have received, and of the necessary medical administration to back it up, which is not insignificant, have both been excellent.
Recent blood tests, which are done at regular intervals, seem to say mostly what one would expect and, in particular, as of mid-October 2019 the prostate-critical blood marker PSA (defined above) is now reduced to 0.56. This marker is a density or mass indicator and is measured in nanograms per millilitre, abbreviated to ng/ml. What it means at a fundamental scientific level I have no idea, but one can readily infer that less is good and much less is better still… the statistical trend in this case is given in the chart attached below. An upper limit is supposed to be 4, I am told, so it is now at least well on the right side having peaked at almost 40 earlier this year. When it hits Zero (not if !) this will become a major positive milestone I expect.
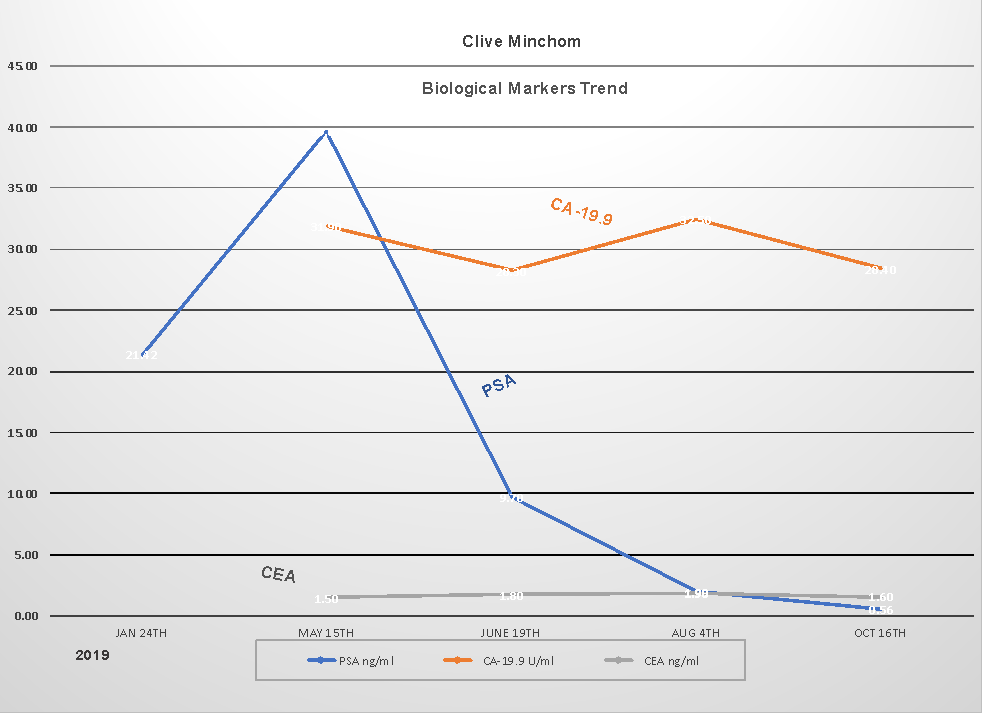 Three cancer indicating “biological” blood markers are shown in the chart above. Other than PSA, which is the marker specific to prostate cancer and has fluctuated wildly as seen in the chart and as described in the paragraph immediately above, the CEA and CA-19.9 blood markers have both remained steady and I believe remain within normal ranges. CEA stands for Carcino Embryonic Antigen and CA-19.9 stands for Carbohydrate Antigen 19.9.
Three cancer indicating “biological” blood markers are shown in the chart above. Other than PSA, which is the marker specific to prostate cancer and has fluctuated wildly as seen in the chart and as described in the paragraph immediately above, the CEA and CA-19.9 blood markers have both remained steady and I believe remain within normal ranges. CEA stands for Carcino Embryonic Antigen and CA-19.9 stands for Carbohydrate Antigen 19.9.
The medical team in charge of my treatment at Rambam has been both decisive in aggressively planning for a total 100% cure, and yet very careful in its implementation, with few side effects to date from either component. What the overall effect the combined radiation and pharmacological treatments completed to date will now have had on all the known malignant areas is obviously now the key question at this point. Also, whether cancerous cells might have spread to other places in the mean-time. To find out, one might suppose that in late January, 2020 i.e. after a three-month interval to let things settle down, there will be more blood tests. Perhaps also another combined PET/CT body scan as was first done last April, which at that time precisely mapped out for the first time all the cancerous areas in the body, including beyond the prostate. To find out will be more than interesting.
Meanwhile the Zytiga “biological” testosterone reducing therapy (also sometimes misleadingly called “hormone” therapy), which began in May, will continue its work of suppressing tumour growth everywhere pharmacologically. I understand this will continue until next summer to keep the lid on things, and eventually hopefully administer the coup de grâce, as it were.
Zytiga is fairly strong stuff, yet has been quite readily tolerated by my body so far, with only occasional quite severe shortages of breath as a significant side effect (there can be several others if you look at the product literature) – though in mitigation that was when playing tennis in 30 degrees celsius and with associated high humidity. In response, now I take the pills after playing tennis instead of before and do a lot of deep breathing exercises on court; it is also seasonally a lot cooler now. Sometimes, between the pills and the radiation, I have gotten really quite tired once or twice, and taken a day or two to recoup. With a 20 cubic centimetre malignant tumour being burned up inside one by a high-powered microwave unit, perhaps this was not altogether surprising.
Otherwise it has been basically business as usual, and the only chore was the 45 kilometre commute to Haifa four days a week, then waiting in line in a busy waiting room, just like one’s Dentist’s, more than thirty times to be irradiated. Indeed “business as usual” is an absolutely essential ingredient for approaching something like this – positive thinking and refusal to let difficult issues get on top of you, together with continued optimism no matter what, as an act of will, are essential emotional attributes in facing what otherwise could be quite daunting to many.
I guess we must just kill these malignant cells before they kill me. And I am much too ornery to let them get there first.
Given the issues involved, and the specialized tests and consultations which all have had to take place in sequence over several months, followed by the extended periods of treatment as well, things seem to happen relatively slowly in cancer treatment. Even so, from initial diagnosis in March to where we are now to, prospectively at least, already a possible near-cure position, that is still pretty quick. Thirty years ago, none of this would have been possible at all. And Oncology specialists have other weapons in their armoury today as well.
Even so, quite nasty adverse surprises could still emerge out of left-field, and one must still carefully respect what remains a highly dangerous, and unpredictable, enemy and stay the course: in a disciplined manner and without sentiment. So, let’s see how this all turns out in January, and the months beyond during 2020.
Finally, the overwhelming impression to date from my experience above is that Haifa’s Rambam Hospital now has a leading clinical position in cancer treatment, one which can stand up to the very best anywhere in the world and they deserve to be supported. Together with its new, adjacent, Eyal Ofer Heart Hospital, its new Children’s Hospital and other projects under way the Rambam is parlaying its multi-disciplinary approach into something quite special.
Clive Minchom
October, 2019
Email: cminchom@mac.com
Mobile: 972 (0)54 626-7304

